![]()
CUREMA is a multi-centre, international public health intervention research project. Our study population is represented by people involved in activities related to artisanal and informal gold mining, who are active and mobile in the Guiana Shield, deep into the Amazonian Forest.
The adventure that started with the Malakit project, has entered a new stage!
Our team has been working for several months on a new project that addresses challenges identified over the past few years: the residual circulation of Plasmodium vivax, the need to further improve the awareness about antimalarial resistance’s risk. The CUREMA project (Radical CURE for MAlaria among highly mobile and hard-to-reach populations in the Guiana Shield) is the fruit of this work , and aims to evaluate a new intervention combining the delivery of Malakits (simplified and improved thanks to TDR/WHO’s support) with a specific action targeting Plasmodium vivax, now the predominant species in our target population. Read the article describing the whole protocol!
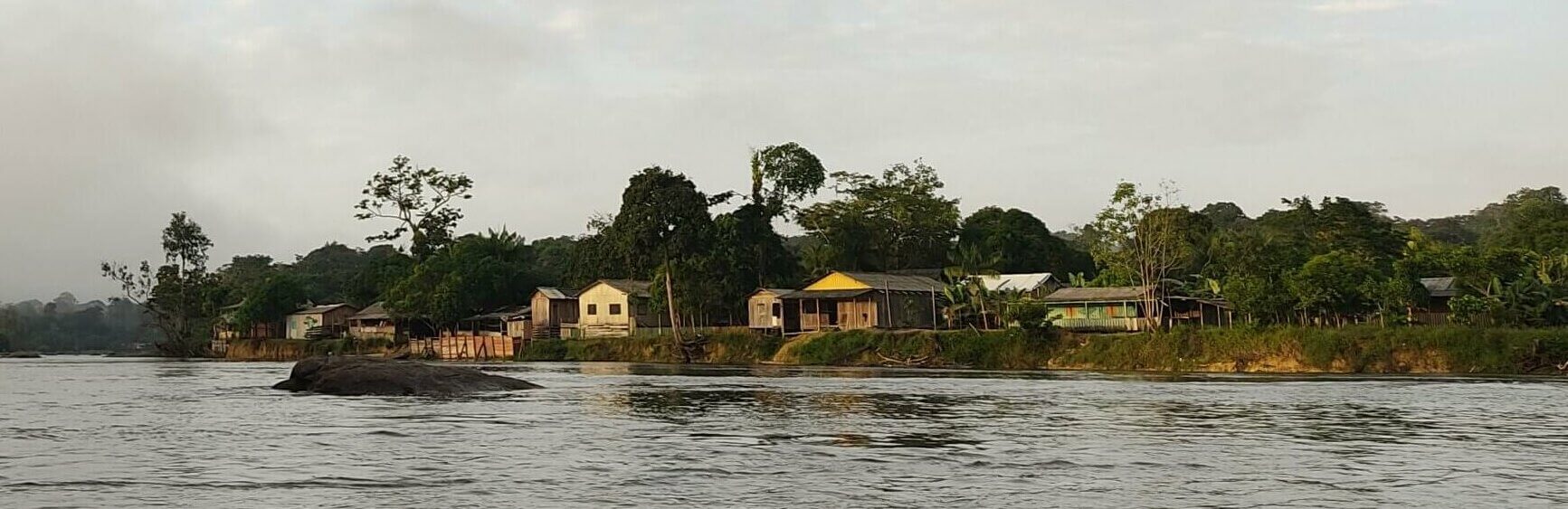
As for Malakit, people involved in activities related to artisanal and informal gold mining (garimpeiros) in the heart of the Amazonian rainforest are CUREMA’s target population: we propose the participation to the garimpeiros moving across the south of the Guiana Shield, between Amapá (Brazil), French Guiana (France) and Suriname. Like during the Malakit project, to overcome the obstacles posed by the remoteness and (often) the informal nature of the activites carried out by our target public, we offer the intervention in the logistical and support hubs (staging areas) of the miners, easily accessible and located in the border regions between the concerned territories.
We will evaluate a complex intervention that includes a common core (malaria health education activity) and two modules that are offered to potential participants:
- The “Radical cure” module is represented by a treatment targeting asymptomatic individuals at risk of carrying P. vivax. The aim of this module is to prevent relapses and to reduce the number of human hosts able to transmit the parasite.
- The “Malakit” module corresponds to the distribution, after appropriate training, of a malakit (self-test and self-treatment kit). The aim of this module is to provide access to quality diagnosis and treatment for episodes of symptoms compatible with malaria that occur in situations of extreme remoteness from health services.
A common core of health education activities focuses on malaria: its causes, means of prevention, the main differences between P. falciparum and P. vivax disease, the importance of a complete treatment against any form of Plasmodium sp. It will be offered individually to participants, during the inclusion process, but also to the community living or transiting the staging areas through collective reach-out activities.
Our purpose is to evaluate a strategy that, if appropriate, can be implemented by health authorities in the region, but also in other countries with residual malaria transmission in populations with similar characteristics.
We therefore keep a pragmatic approach, so that conclusions of the study could be transferred as smoothly as possible to real life, while at the same time focusing on the safety of the
intervention. Thus, the study field workers who will administer the intervention are facilitators belonging to the target community and with a similar profile to that of health workers recruited by many malaria control programmes, particularly in remote areas. In addition, follow-up is simplified, and follow-up data maybe collected both through face-to-face visits and remotely administered questionnaires (by phone or through a specific mobile phone app).
In order to generate data necessary for health authorities to potentially take over the intervention in the future, the study evaluates two aspects of the intervention: effectiveness and implementation. 
- First, we want to evaluate the population-scale effectiveness of the intervention to reduce malaria transmission with a quasi-experimental approach.
- Secondly, we will analyze the implementation of the intervention, and generate valuable knowledge for further implementation within local health services.
This evaluation will be carried out through the components of the CUREMA study:
- the data produced by the intervention itself,
- the pre/post-intervention cross-sectional surveys,
- the contribution from the social sciences and community-based approach (qualitative research and participatory evaluation process),
- the modelling of epidemiological surveillance data.
Many of the components of the intervention and evaluation have been co-designed with a participatory approach together a variety of actors and through community engagement.
This project began in 2022 and ended during the first quarter of 2025.
Sponsor : Centre Hospitalier de Cayenne
Investigator coordinators : Dr Alice SANNA, Pr Maylis DOUINE, Dr Yann LAMBERT (France)
Investigator Principal Suriname : Dr Stephen VREDEN
Investigator Principal Brazil : Dr Martha SUAREZ-MUTIS