The CUREMA project aims to evaluate an innovative intervention targeting the elimination of malaria in a population located far from the healthcare system. This intervention is complex, and involves proposing the actions described below to this population. The strategy used to propose these actions is also a key element of the intervention:
- Offering the intervention on an ongoing basis, rather than in one-off operations;
- Offering it at points where the target group’s cross-border mobility passes through, at the entrance and exit of the gold-mining sites, due to the difficulties (logistical, administrative, security) of accessing the sites themselves;
- By professionals characterized by their proximity to the target population (almost a peer intervention);
- With close supervision and support, to optimize the quality and reliability of the intervention.
What is it?
The CUREMA project intervention includes a common core (health education activity on malaria) and two modules that will be offered to participants. Each participant meeting the inclusion criteria will be able to choose to take part in one or both modules.
The “Radical Cure” module
The treatment targeting asymptomatic individuals at risk of carrying P. vivax aims to prevent recurrences and reduce the number of human hosts capable of transmitting the parasite, due to relapses that could occur both in the forest and when the carrier returns to rural/urban areas. The asymptomatic carriage of P. vivax, as well as its relapses (responsible for approximately 80% of malaria attacks linked to this species worldwide), are in fact often responsible for maintaining or re-seeding transmission of the parasite.
The “radical cure” consists of a 3-day course of chloroquine combined with a 7-day course of primaquine or a single dose of tafenoquine (see the kit “radical cure” here)

The radical cure can be offered to people leaving or planning to enter gold-mining areas.Individuals at risk will be identified based on clinico-epidemiological criteria:
- their history of recent malaria (biologically confirmed or simply declared)
- their exposure to high malaria circulation areas over the past year.
The presence of contraindications to the proposed treatment is also explored, in order to define the participant’s actual eligibility to receive the treatment.
These information are collected via the inclusion questionnaire (history of adverse events or known intolerance, serious psychiatric history) and rapid tests carried out at the inclusion site (pregnancy test, semi-quantitative assessment of G6PD activity levels using the SD Biosensor ).
Participants who have received the radical cure benefit from active follow-up during the two weeks following their inclusion (on day 3, day 6 and day 15). In order to adapt to the mobility of the target population, follow-up is offered in the form of three alternatives (which may be cumulative):
 face-to-face follow-up on the study premises;
face-to-face follow-up on the study premises; - by telephone call made by the facilitator who ensured inclusion;
- by a mobile application (link to the app page), specifically designed for offline data collection, to monitor all those who travel to remote areas in the days following the start of treatment.

 The “Malakit” module
The “Malakit” module
 The
TheIt consists in the distribution, after appropriate training, of a malakit (self-testing and self-treatment kit).
This kit provides access to quality testing and treatment for episodes of malaria symptoms that occur in situations of extreme remoteness. The purpose is to:
- prevent the emergence of antimalarial resistance due to inappropriate treatment,
- reduce the duration of contagiousness of symptomatic malaria attacks occurring in the forest,
- reduce the risk of complications from malaria treated late or incompletely.
To be eligible for this module, participants must be planning to enter an illegal gold-mining site in French Guiana within the following month, and among them, must have understood the training on the use of the kit given during inclusion.
This module is inherited from the positive experience of the Malakit project and has been simplified and improved (both in terms of delivery process and layout) thanks to the support of TDR/WHO and the experience of the Suriname Ministry of Health.
A common core of health education will cover malaria: its causes, means of prevention, the main differences between P. falciparum and P. vivax diseases, the importance of complete treatment against all forms of Plasmodium sp. It will be offered individually to participants, during the inclusion process, but also to the community living in or transiting through the staging areas, through collective awareness-raising activities.
When ?
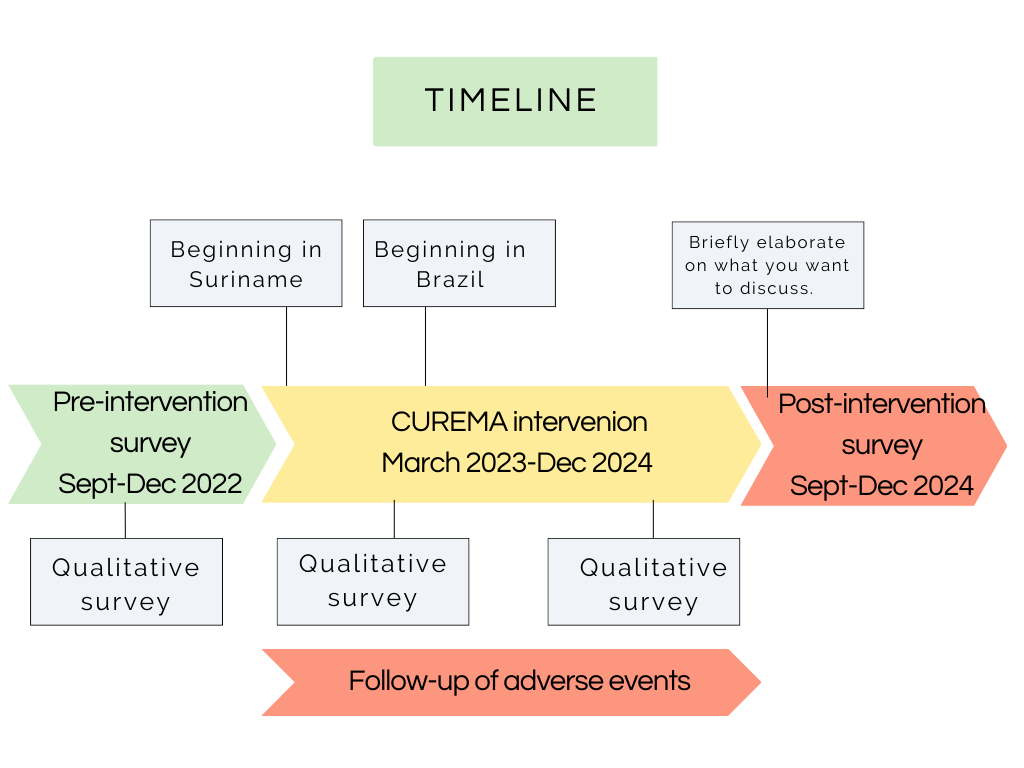
Implementation of the intervention began in the field in March 2023, and is being carried out gradually in all the project’s inclusion sites. We plan to continue the intervention until the end of December 2024.
Where ?
The CUREMA project intervention is proposed in localities usually frequented by gold miners as they leave or enter gold-mining areas in French Guiana, Suriname or Brazil. The intervention sites are identified by an orange dot on the map below.

For whom?
The conditions for participating in this stage of the CUREMA project are the following:
- be involved in activities related to gold mining (either have worked in the artisanal gold mining sector within the last 12 months, or plan to enter a gold mining site within the next month)
- be at least 18 years old,
- weigh more than 35 kilos,
- have no symptoms of malaria at the time of inclusion.
People with these characteristics may be offered participation in the intervention initially. They will then receive one and/or the other of the two modules, depending on:
- Their wishes
- Their specific eligibility for the chosen module, investigated during the inclusion process, as described above.
By whom ?


Participation in the intervention is made possible in the field by the project’s ” facilitators “, professionals recruited for the study by the SWOS Foundation in Suriname and by the DPAC association in Brazil, whose main characteristic is their proximity to the study population.
They belong to the community linked to gold mining, or know it closely, and live in one of the localities of the study. Their professional profile is similar to that of community health workers involved in malaria control in the countries concerned by the intervention. In Suriname, thanks to a partnership between the SWOS Foundation and the National Malaria Elimination Program, some of the facilitators share their time between the CUREMA project and MSD (malaria service deliverer) activities. The choice of this personal and professional profile is motivated by a desire to increase the transferability of the project to National Programs in the event of a successful experimental phase.
Before starting their work with the project, the facilitators received basic training in malaria and malaria control. They also took part in a 3-week theoretical and practical training course, enabling them to master study procedures and the principles of health research.
