Objective and principle of the intervention
The objective of the intervention is to provide the study population with the equipment and resources needed to handle an episode of malaria symptoms by themselves, when they are in an isolated location.
All the participants are offered training, and for those who have a smartphone, an application, to:
- understand the purpose and rationale of the whole project, the importance of correct use of the kit, and receive additional information about malaria and how to prevent it,
- learn how to perform a self-diagnostic test, read and interpret the results, and treat themselves accordingly and appropriately.
NB: The consent to download the application is independent of consent to participate in the study.
The expected outcome is that participants obtain better knowledge and change their attitude and behavior towards malaria prevention and case management.
Who carries out the intervention?
Malakit facilitators are responsible for training participants, sharing the application, handing out Malakits and LLINs for hammocks, and replenishment or replacement of Malakits.

Malakit facilitators
They are also in charge of the investigation itself : they enroll participants in the study and collect data during the enrollment phase and subsequent visits. They are also tasked with assembling kits and stock management.
There are two facilitators per distribution site on the river borders, and one in Paramaribo.
Off-site missions at other rest sites on the Maroni river have also been carried out, according to gold mining activity and flows of gold miners.
Facilitators are recruited for belonging to or being close to the community of garimpeiros, their fluency in the Portuguese language, and their IT literacy for tablet and smartphone use.
Among the desired but not mandatory recruitment criteria were:
- experience as a health worker or as a surveyor, or in social or health mediation,
- and the ability to speak English or French.

Theoretical training
- The facilitators first received general training about malaria, followed by theoretical training on their duties, and practical training on the field. The Malakit theoretical training course included:
-
- Context and objectives of the project
- Rationale and novel aspects of Malakit
- Rights of participants and informed consent
- Training carried out as part of inclusion
- Data collection using questionnaires : First visit and return visits
- Kit assembly and stock management
-
- Secondly, they all received formal or informal theoretical training after the first return visits, to master the questionnaire administered at that stage.
- Formative supervision on the field enabled facilitators to be trained on application sharing once the application was finalized and in the updated version of the return visit questionnaire, and made it possible to recap several crucial points.
What are the steps to enrolling subjects in the Malakit study?
TRAINING
Training can be carried out by one or two facilitators. The recommended number of participants per training session is one to four, but in exceptional circumstances, that number can rise to five or six.
1/ Check eligibility criteria:
-
- Being at least 15 years old, with presence of a legal guardian if aged between 15 and 17. The cut-off age was determined by taking into account the ability to use the kit on oneself, the minimum weight for the dosage of medication supplied in the kit, and the known presence of minors in the camps.
- Working or accompanying someone working illegally in gold mines in French Guiana, or intending to work there or accompany someone.
- Not being already enrolled in the Malakit study.
2/ Provide information on the project to the potential participant(s) including the following messages:
-
- The enrollment process takes about one hour
- Participation involves pricking oneself on the finger
- Participants must sign a consent form


3/ Show the Malakit animated video
4/ Display the kit
5/ Conduct short discussions about malaria with participants:
Starting with one of the following questions:
-
- “Have you already had malaria?”
- “What were the symptoms?”
- “Do you know how malaria is transmitted?
- “When you have fever and/or headache in the forest, what do you think it is?”
- “What other symptoms of malaria did you have or do you know?”
6/ Provide explanations using illustrated posters
-
-
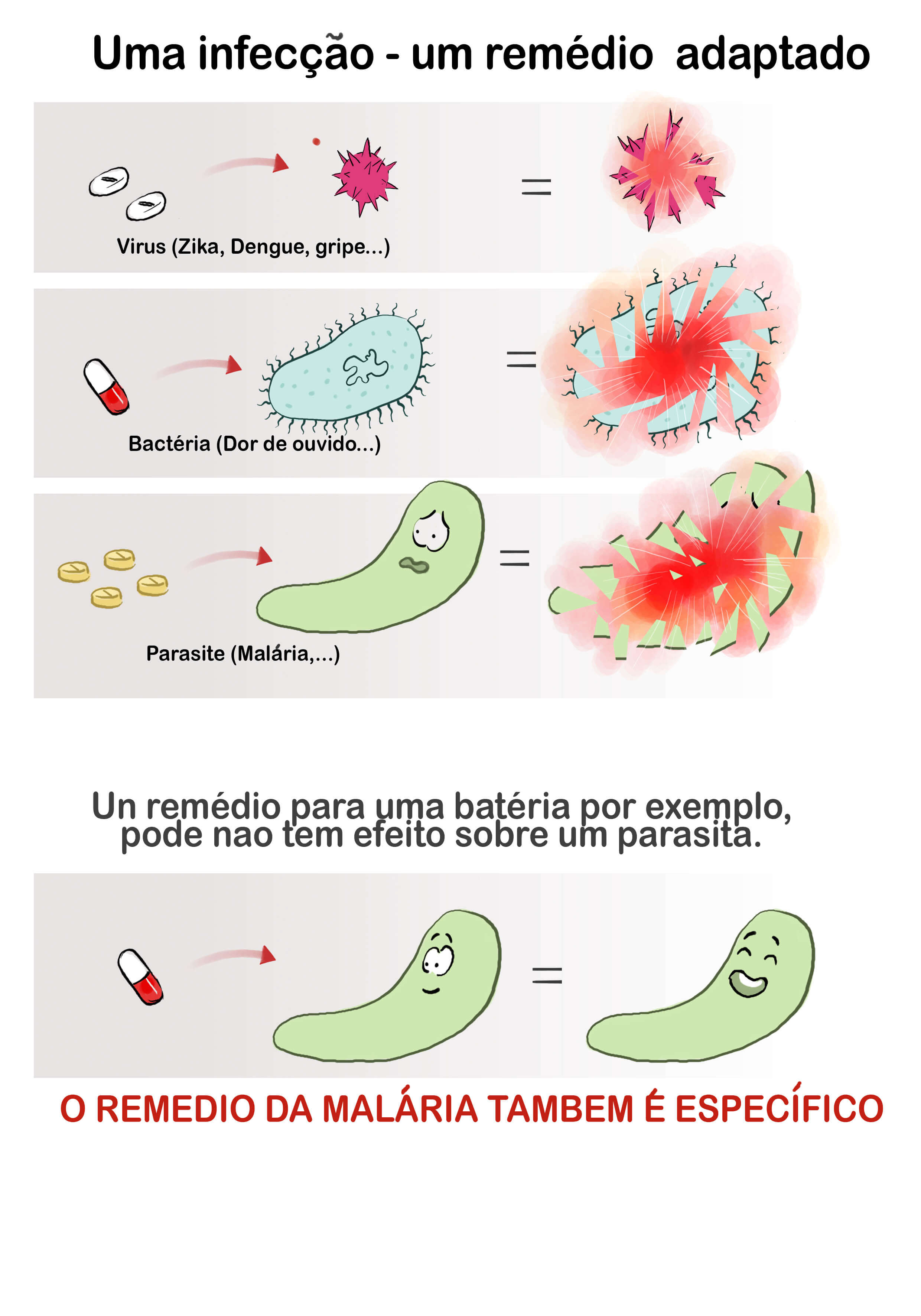
“One infection – one appropriate treatment”: The message is that if the treatment does not correspond to the cause of the infection, it will not work, hence the importance of knowing the cause of the infection.
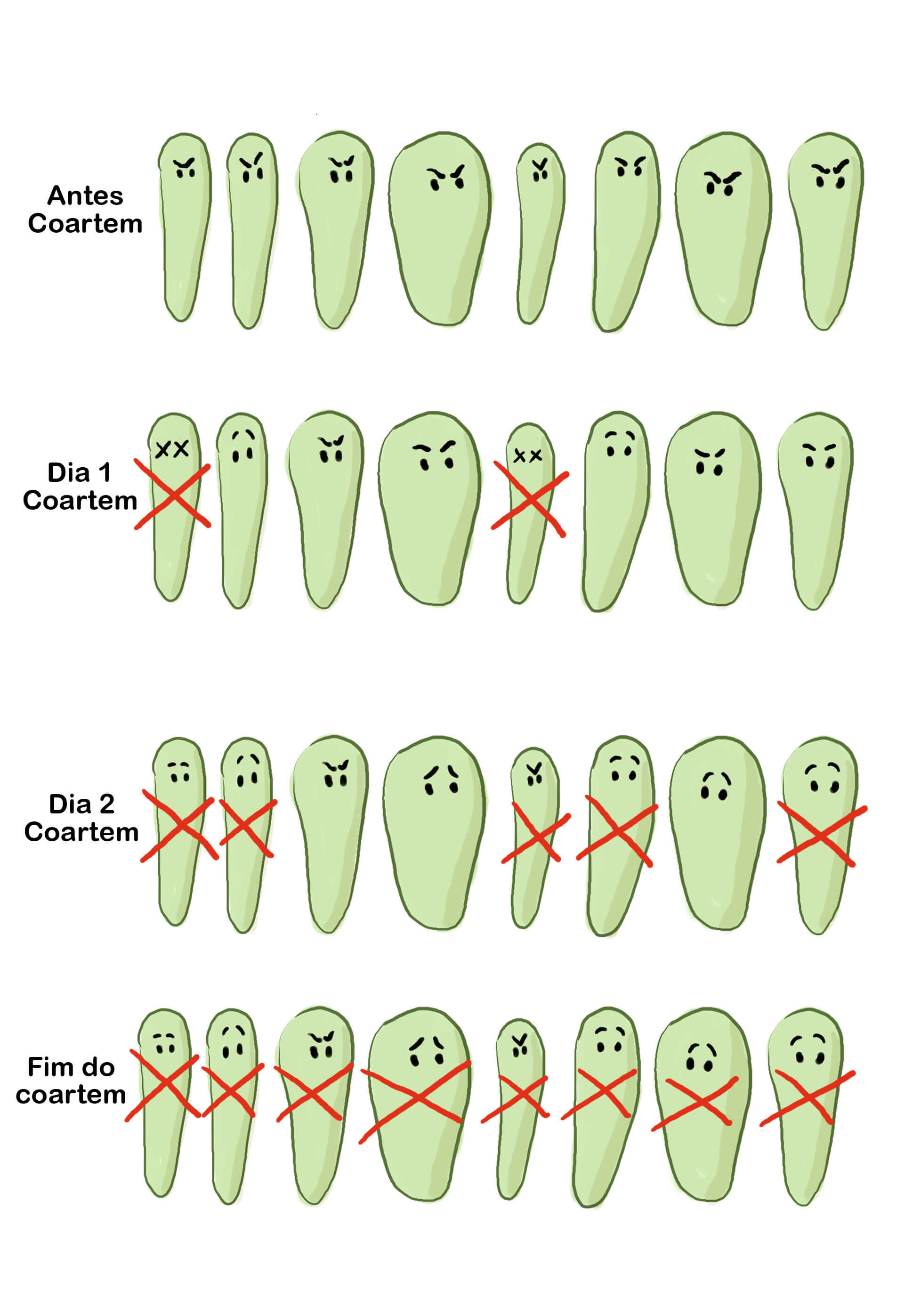
- Poster of parasites (not mandatory, and not used by all facilitators): the message is that a 3-day course of artemether/lumefantrine is needed to eliminate all parasites, even the strongest.
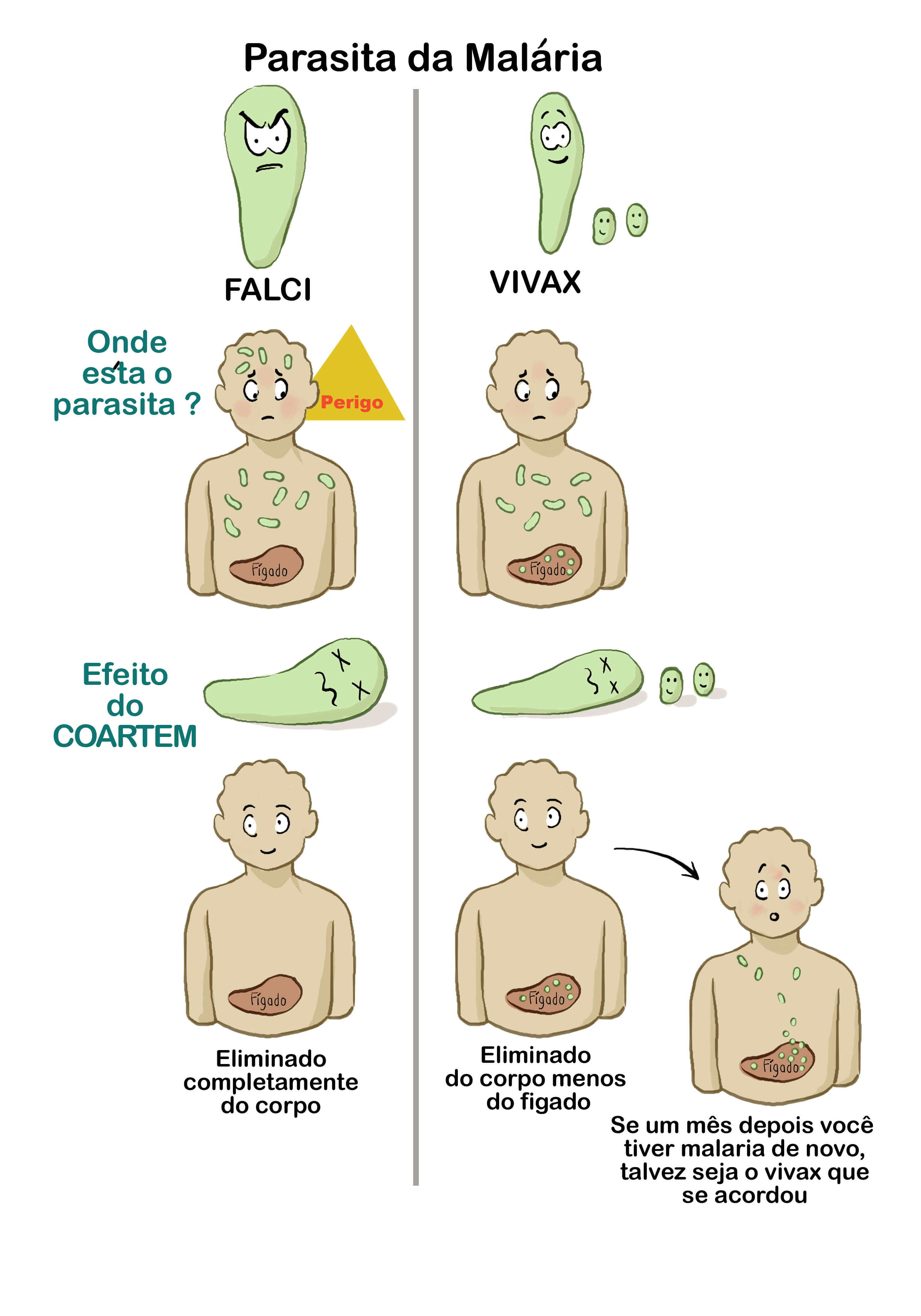
- “Malaria parasite”: explanation about the existence of P. vivax and P. falciparum, their difference, and the usefulness of the RDT and treatment provided in the kit for each. The main objective of this poster is to encourage participants to seek professional health care when symptoms come back one month after the end of the kit treatment i.e. in case of P. vivax relapse.
- High-risk situations : severe signs and contraindications: the message is that in case of one of the illustrated situations, the participant must start the Malakit treatment, and at the same time seek medical care as soon as possible.
-
7/ Show the video “How to self-administer a RDT”
8/ Guide the participant as they perform a step-by-step, self-administered RDT:

With the help of the printed illustrations on the kit, and then interpret the results ⇒ Self-administration of the entire RDT process is one of the inclusion criteria. If the test is positive, the participant will be referred to the nearest malaria care service.
Note the corresponding time and first name on each test device.
9/ Explain how to take the Malakit medications according to the test result.
This includes the concept of resistance and the importance of finishing the entire course of treatment, even if the person feels better. Contraindications for taking primaquine, such as being pregnant or breastfeeding, are also explained, using the illustration on the kit.
ENROLLMENT PROCEDURE AND ADMINISTRATION OF THE QUESTIONNAIRE
1/ Deliver the information note and allow the participant to ask questions.
2/ Fill out the paper informed consent form in two copies:
One for the participant and one for the investigator.
3/ Administer the questionnaire on the tablet:
-
- Check the final inclusion criteria:
- ability to read and interpret test results
- understanding of when and how to take the treatment correctly

- Attribute a unique ID number, with a bar code and letters/numbers format. One ID number label is stuck on the informed consent form and another identical label is stuck on a plastic card to be used as a “Malakit ID card” by the participant to preserve anonymity. The bar code is scanned using the tablet.
- Collect sociodemographic and intervention data: test result, previous possession of a kit, scan of the kit number distributed and of the application ID code, whether or not a mosquito net was distributed.
- Check the final inclusion criteria:

4/ Hand out the “ID card”, the LLIN, and the malakit with the following messages:
“It is important to come back to a distribution site if you have used the kit”; “Keep the ID card and the kit separately”; “Bring back the kit and ID card and the RDT waste at each new visit”.
POSSIBLE VARIATION
The components of the Malakit smartphone application can be used as training support tools. For example, how to read the RDT can be explained using the interactive part of the application, enabling participants to be trained in the use of the application at the same time.
Possibilities for tailoring interventions to individual participants
Certain characteristics of participants , listed below, can lead to adaptations by the facilitator:
- Number of participant(s) per session
- Available time
- Interest and ability to concentrate
- Reading ability
- Smartphone ownership
- Smartphone literacy
Adaptations will influence the level of information given, the rapidity of explanations, and the number of repetitions of important messages.
For example, full explanations of the application will only be given if time is available and if the participants have sufficient smartphone literacy.
What are the steps to follow for a return visit?
Here is the procedure when a participant comes back to a distribution site:
1/ Check that the person has been already been included in the study by:
-
- Checking for the presence of the ID card and/or the kit
- Asking where, when, and by whom they were enrolled
- Optional: Asking the participant to perform a self-administered RDT in front of the facilitator
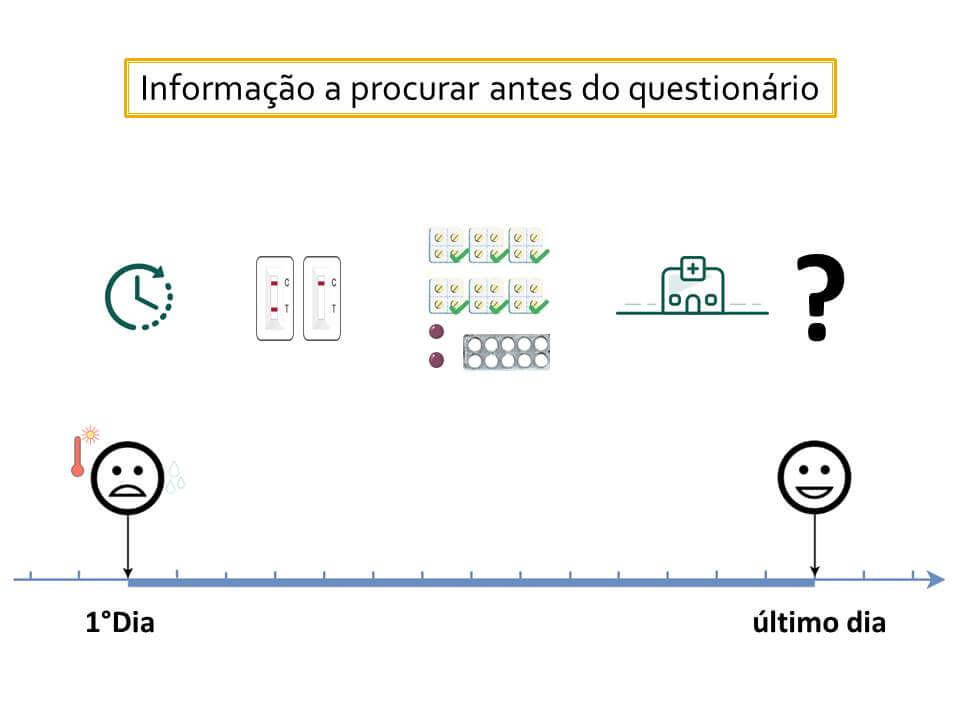
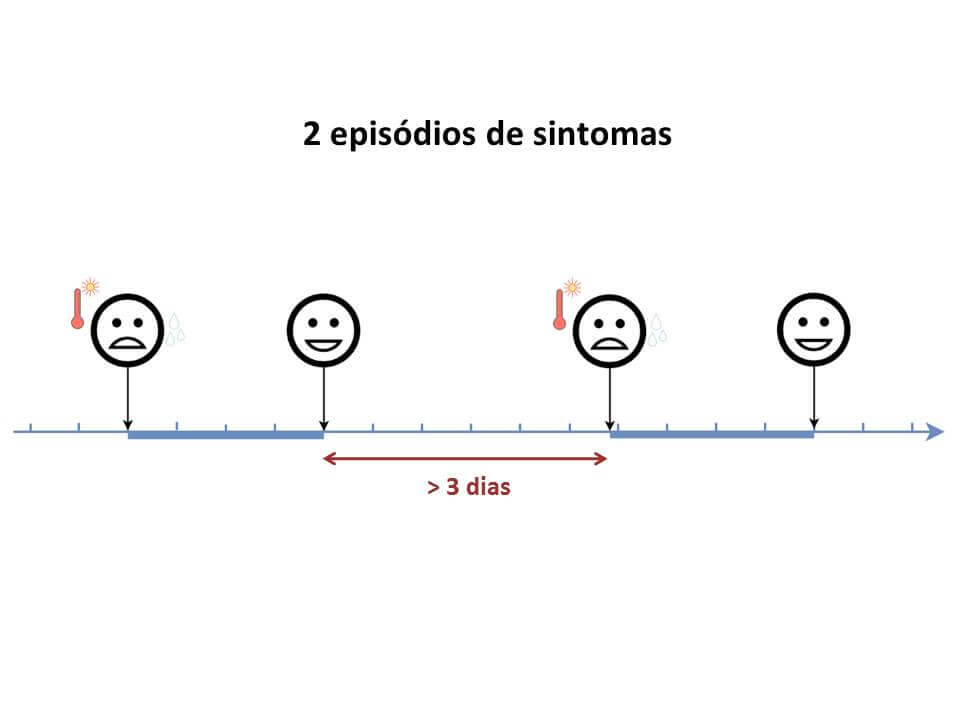
2/ Debrief the participant on what has happened since the last visit at a distribution site:
The facilitator asks if there have been episodes of symptoms and if there has been use of the kit without symptoms, including use of the kit by someone else.

- If the participant has a smartphone but does not have the application yet, the facilitator shares the application.
- If the participant no longer has an ID card , the facilitator attributes a new ID number to the participant and fills out a “missing ID number form” where they stick the new ID number. A new card is delivered with this ID number.
- If waste (used RDT) has been brought back, the facilitator writes down the ID number of the participant on the waste bag and keeps it safely for future quality control.
3/ Replace or replenish the kit if necessary.
4/ Administer the return visit questionnaire.
NB: The facilitator has the right to refuse to replenish or provide a new kit if they find out the person is being deceitful and only wants to obtain kits to sell.